
Clinician's Guide
to using MEPA in UNHS
Using MEPA in UNHS Programs
The purpose of univeral newborn hearing screening (UNHS) is to detect hearing loss as early as possible to start treatment as soon as possible, which is crucial for speech and language development. Studies show that about 80% of screening refers are due to fluid or other blockages in the ear from the birth process that are temporary. These babies eventually pass their DPOAE test if the fluid or other problem in the ear clears on its own. The MEPA test will help determine when the middle ear is clear, so that screening results can be more clearly interpreted.
Hunter et al. (2010) and Sanford et al. (2009) showed that MEPA reflectance was more sensitive to DPOAE status than 1 kHz tympanometry.
Norms based on ears with DPOAE pass and DPOAE refer status
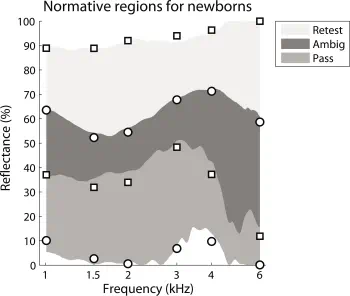
(Fig 3, Hunter et al., 2010)
Interpretation
In both HearID and OtoStat, the normative region for newborns is based on Figure 3 from Hunter et al., which is for infants aged up to 4 days old with normal DPOAEs. The pass region is defined as the minimum reflectance for the group with normal DPOAEs (DPOAE pass result) and the tenth percentile for the group with abnormal DPOAEs (DPOAE refer result).
- If the MEPA reflectance function falls above the "DP-pass" normative patch, especially around 2 kHz, outer or middle ear problems may be the cause, and rescreening after a few hours or a day is recommended prior to diagnostic referral. If the infant refers again, prompt referral for diagnostic testing is needed.
- If the MEPA reflectance function falls within the "DP-pass" normative patch, especially around 2 kHz, the middle-ear is more likely to be normal and associated with a DPOAE pass result. If the DPOAE result is ambiguous or a refer, then middle ear issues are not suspected as the cause. Prompt referral for diagnostic testing is needed.
How to interpret DPOAE and MEPA Reflectance results in a newborn
| Overall DPOAE result | Reflectance at 2 kHz |
|---|---|
| pass | in pass region |
| Interpretation: pass - normal result | |
| pass | above pass region (i.e., in the ambiguous or retest regions) |
| Interpretation: pass - may have middle-ear issues, but cochlear response is normal | |
| refer | in pass region |
| Interpretation: refer - consistent with SNHL - needs follow-up referral | |
| refer | above pass region (i.e., in the ambiguous or retest regions) |
| Interpretation: re-screening is indicated. Repeat MEPA to determine if middle ear issue is resolved. | |
Tone or chirp stimuli?
The frequency region around 2 kHz is the most diagnostic. In HearID, you can either run a test using the default chirp, or you can change the stimulus protocol to use a 2 kHz tone. The benefit to doing this, especially if you test primarily infants, is that the tone test is faster and achieves a higher signal-to-noise ratio. However, you lose potentially interesting information at other frequencies. OtoStat 1 and 2 uses only a chirp stimulus. OtoStat 3 can use a tonal stimulus in addition to the chirp (which is used to calibrate the level of the tone).
How to run this test
OtoStat 3
- Ensure the patient birthdate is entered accurately in OtoStation.
- Run the DP_InfantScreen_unilateral sequence (MEPA and DPOAE test). If the patient is a newborn infant, the results show automatically.
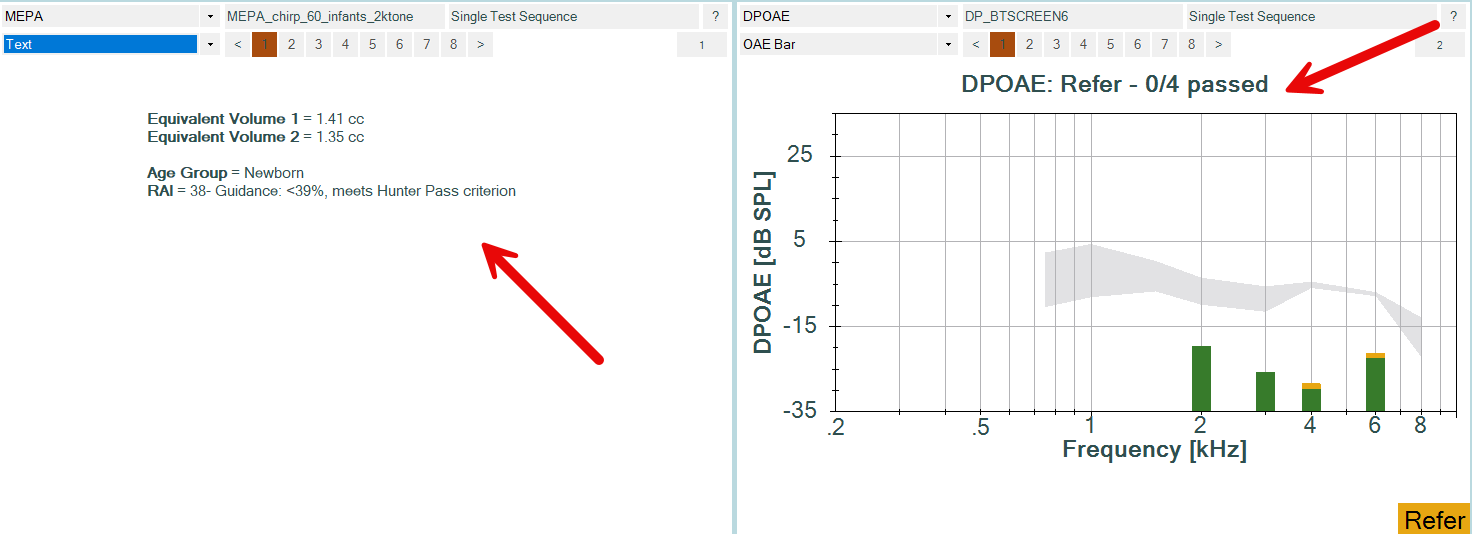
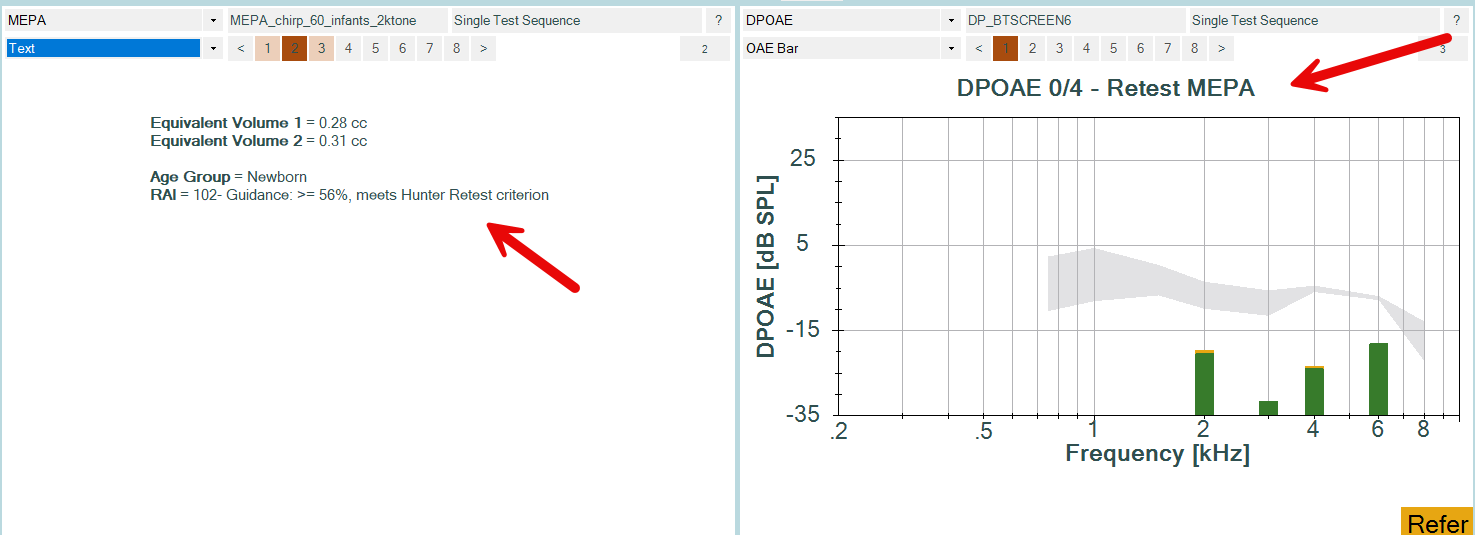
- The RAI is displayed in the MEPA "Text" panel along with pass/refer guidance . Use the dropdown menu on a MEPA plot space to choose the "Text" display, if it is not already showing.
- The DPOAE plot title shows the overall result: DPOAE Pass, DPOAE Refer, or DPOAE - Retest MEPA. This interpretation uses the MEPA RAI result to differnetiate a true refer from a false-positive refer result. If the DPOAE plot is not showing, use the dropdown menu on a DPOAE plot space to select the "OAE Bar" plot.
OtoStat 2
The MEPA test is run immediately prior to the DPOAE test, using the same equipment and the same probe fit. No uncomfortable ear-canal pressurization is needed.
Ensure the "MEPA chirp 60" and "BTSCREEN6" protocols are selected. The MEPA and DPOAE test are run automatically and displayed on-screen together when choosing the "Newborn <6m" button. Infant norms for the MEPA chirp stimulus are from Hunter et al. (2010) and are automatically displayed. Norms for the DPOAE test are Boystown 90% ambiguous region.
Tap on the screen to advance to the analysis screen, or download to review or print the test in OtoStation. The Reflectance Area Index (RAI) at 2kHz is displayed. Interpretation depends on the DPOAE results (see table above).
OtoStat
The MEPA test is run immediately prior to the DPOAE test, using the same equipment and the same probe fit. No uncomfortable ear-canal pressurization is needed.
Ensure the "MEPA chirp 60" and "BTSCREEN6" protocols are selected. The MEPA and DPOAE test are run automatically and displayed on-screen together when choosing the "Newborn <6m" button. Infant norms for the MEPA chirp stimulus are from Hunter et al. (2010) and are automatically displayed. Norms for the DPOAE test are Boystown 90% ambiguous region.
On the print summary, the Reflectance Area Index (RAI) at 2kHz is printed out along with the associated status: pass, ambiguous, or retest. Interpretation depends on the DPOAE results (see earlier table).
HearID v5.x
Run the DPOAE BTSCREEN4 or BTSCREEN6 test.
For MEPA, choose the "Infant 2kHz screen" protocol by clicking on the MEPA Param button, selecting "tone" from the stimulus field and then choosing it from the "tone protocol" field. Or equally, choose "Stimulus Parameters" from the MEPA menu in the main HearID window.
Optimize the display to show the results for the tonal stimulus by choosing the "2 kHz Infants" display option in the "Display Preferences" on the MEPA menu.
If you wish to make other modifications to the display, note that the chirp or tone norms can be selected from the Normative Data panel. Choose "MA Infants" or "MA Infants 2 kHz" from the dropdown menu. After making your modifications, save as a new display parameter set.
HearID v3.x
- Run the DPOAE BTSCREEN4 or BTSCREEN6 test.
- For MEPA, either use the default chirp stimulus, or set up the 2 kHz tone stimulus manually by following the instructions in the manual. Use the settings: sound pressure level (dB SPL)=60, measurement time (s)=1, and target freqs=2000.
- Review the reflectance function graphically, or export the results to an Excel or Matlab file.
- A reflectance result at 2kHz greater than or equal to 56% meets the Retest criterion. Reflectance results this high are typically due to transient middle-ear issues and tend to produce false-positive DPOAE refer results.
- A reflectance result at 2kHz between 39 and 56% is ambiguous, and should be retested if the DPOAE result is a Refer.
- A reflectance result at 2kHz less than 39% meets the Pass criterion. If the DPOAE result is a refer, refer for follow-up.
- You can choose to adjust the frequency range displayed and saving a new display protocol by following the instructions in the manual.
Further reading
Lapsley Miller, J. A. (2015) Why WAI?. OAE Portal Guest Editorial Jun-Oct, 2015. (Read on OAE Portal). Includes case examples from a UNHS program.
Hunter, L. L., Feeney, M. P., Lapsley Miller, J. A., Jeng, P. S., and Bohning, S. (2010). "Wideband Reflectance in Newborns: Normative Regions and Relationship to Hearing-Screening Results," Ear & Hearing 31, 599-610.
Hunter, L., and Shahnaz, N. (2013). Acoustic Immittance Measures: basic and advanced practice. (Plural, San Diego, CA).
Sanford, C. A., Keefe, D. H., Liu, Y. W., Fitzpatrick, D., McCreery, R. W., Lewis, D. E., and Gorga, M. P. (2009). "Sound-conduction effects on distortion-product otoacoustic emission screening outcomes in newborn infants: test performance of wideband acoustic transfer functions and 1-kHz tympanometry," Ear & Hearing 30, 635-652.
Keywords
infant hearing screening, newborn hearing screening, INHS, Universal Newborn Hearing Screening Programme, sensorineural hearing loss, middle-ear wideband reflectance.
Disclaimer
This guide was compiled by Mimosa Acoustics from peer-reviewed scientific research to assist clinicians in interpreting results from HearID and OtoStat. It will be updated as new research becomes available. HearID and OtoStat do not provide diagnoses. All diagnostic decisions are the responsibility of the clinician.
Version 1.3, 13 Dec 2024 (Updated for OtoStat 3).
Prepared by Judi Lapsley Miller, PhD
Version 1.0 was reviewed by Lisa Hunter, PhD, FAAA, Scientific Director, Audiology, Cincinnati Children's Hospital, Associate Professor at University of Cincinnati, 11 July 2013.